

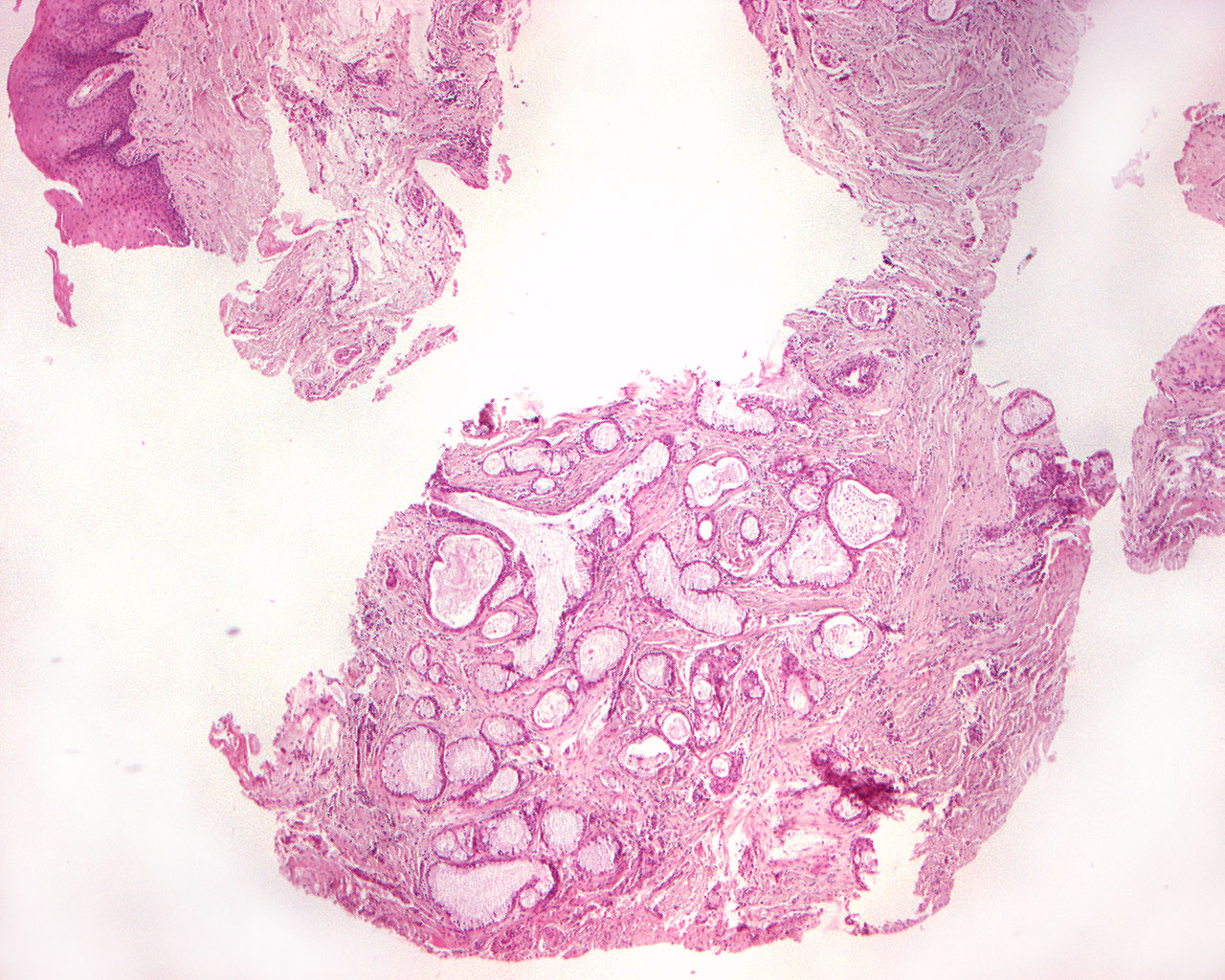
Mucoepidermoid carcinoma (40X)
Clinical information: A 65-year-old woman had had a lump on the left side of the floor of her mouth for a long time. The condition had been perceived as sialolithiasis, but the oral surgeon could not find stone formation. Tumor was removed under tentative diagnosis: Fibroma.
Clinical diagnosis: Fibroma?
Microscopic examination: One can find pieces of mucosa with a convex surface covered by regular, somewhat hyperplastic, multi-layered squamous epithelium. In the subepithelial loose connective tissue, there is diffuse mild to somewhat intense infiltration of mononuclear inflammatory cells. A little deeper, a non-encapsulated, epithelial tumor tissue is seen, mostly made up of irregular lumina of varying size, largely lined by tall, mucous cells and with some mucus content (basophilic substance) and cellular debris centrally (French: débris = fragments). Peripheral to the mucous cells, there is some multilayered squamous epithelium. The stroma is moderately abundant with scattered mononuclear inflammatory cells. Tumor tissue extends all the way to the resection margin in deeper part of the speciman.
Comment: The large content of glandular structures indicates a relatively high differentiation, but the lack of capsule and infiltration right up to the resection margin is emphasized (differentiation, from Latin: dis = apart; ferre = carry, lead): development in different directions; structural and/or functional modification of tissues or organs during development. I general, a highly differentiated tissue closely resembles the maternal tissue, is more benign than a poorly differentiated tissue). A mucoepidermoid tumor with a large squamous component is relatively poorly differentiated (does not have the same structure or function as normal glandular tissue).