

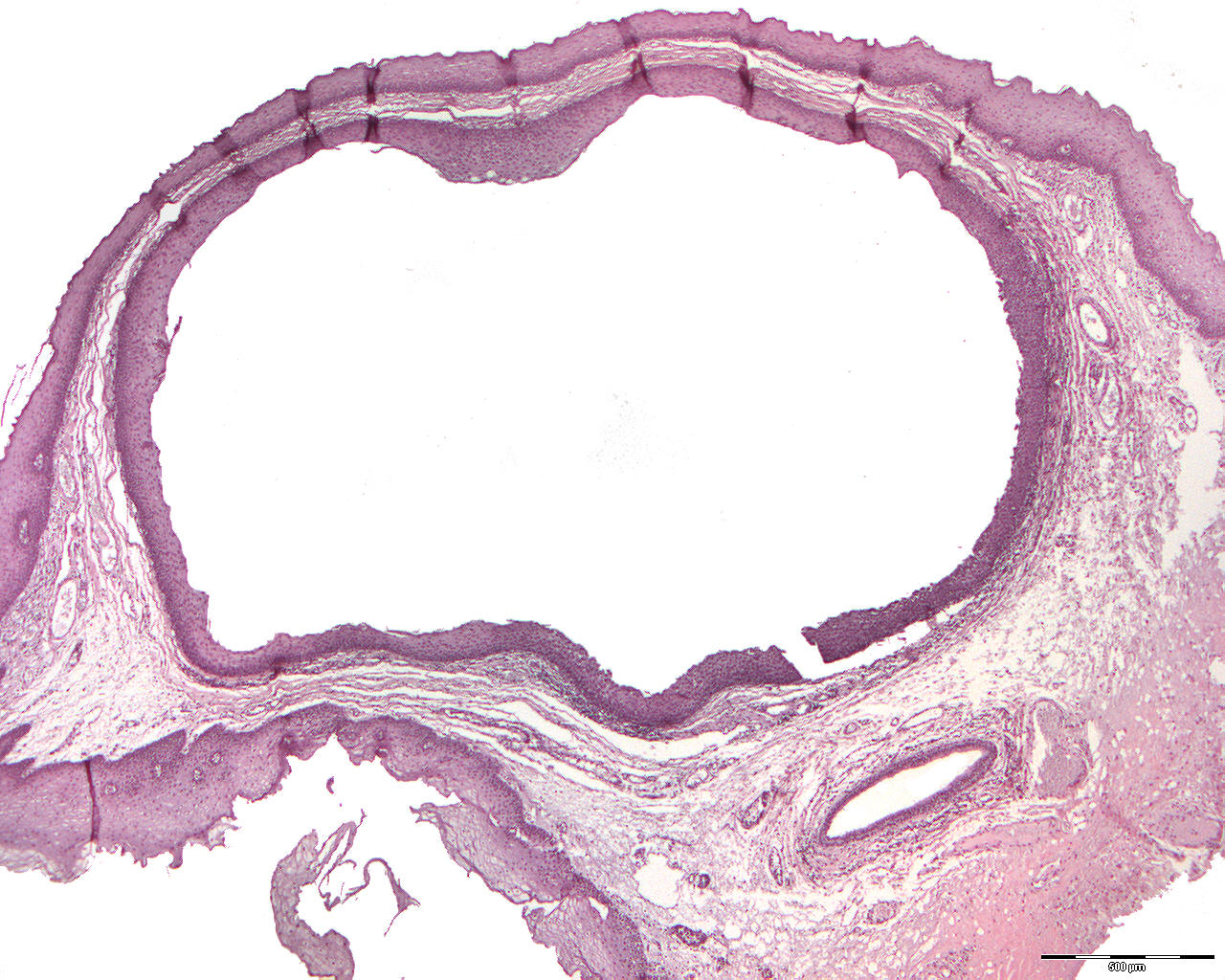
Mucous retention cyst (retention mucocele) (40X)
Clinical information: A 27-year-old woman presented herself with a yellowish, pea-sized tumor on the right side of the floor of the mouth.
Clinical diagnosis: Lipoma?
Macroscopic examination: A broad-based piece of soft tissue with a slightly convex, yellow-white surface with a diameter of 8 mm. The tissue did not float in formaldehyde solution (fat tissue has a lower density than water). When cut, a yellowish-white, hard fragment (sialolith; sialon (G) = saliva; lithos(G) = stone) appeared, which could easily be removed from a lumen surroundet by a thin wall of tissue.
Microscopic examination: A piece of mucosa with a convex surface covered with hyperparakeratinized, regular, multi-layered squamous epithelium can be seen. Centrally, the epithelial covering appears atrophic. Subepithelially, loose, fibrous, edematous connective tissue is seen with scattered mild to moderate accumulation of lymphocytes and some plasma cells. Just subepithelially one can see a lumen lined by relatively narrow, largely unkeratinized, but in some places parakeratinized, multi-layered squamous epithelium that communicates with an excretory duct. This lumen is compatible with the macroscopically described one, which contained a hard tissue fragment (sialolith). Deeper, one finds part of an excretory duct from a salivary gland lined with pseudostratified columnar epithelium.
Decalcified material showed small fragments of yellowish / eosinophilic substance with longitudinal basophilic lines (lineages, lamellar structure) and more basophilic pieces (sialolith). In this case, salivary stones have caused dilatation of a salivary gland excretory duct (a retention cyst).
Comment: As the development of a retention cyst arises from the expansion of an existing structure (salivary duct), it is per definition no true cyst. How is a true cyst defined?